STAR-Malawi rolls out social harms reporting systems in readiness for HIVST

A community stakeholder making a presentation during a workshop in Machinga district
How do we know that introducing HIV Self-Testing (HIVST) will not increase occurrence of social harms and serious adverse events such as physical violence, sexual violence, verbal violence, psychological violence and even death and attempted suicide in villages where HIVST will be introduced? To answer this question, a community engagement system will be developed in the participating villages surrounding health centres that were randomly selected for HIVST kits distribution in the four southern districts of Blantyre, Neno, Mwanza and Machinga. The STAR general population Community Engagement (CE) team in Malawi has rolled out the process of developing the engagement system to capture the social harms across the four districts.
The CE team comprised of two Research Assistants: Wakumanya Sibande and Mwiza Sambo from Malawi-Liverpool-Wellcome Trust (MLWT), a clinical research institution based in Blantyre which is responsible for the research component of Self-Testing Africa Malawi (STAR-M). The first districts to roll out the activity were Neno and Machinga. The activity mainly aimed at conducting a situation analysis/stakeholder mapping in the participating villages, which included exploring existing community reporting structures in the villages, identifying different key stakeholders working in the villages and their interests. The activity also aimed at developing prototype social harms reporting systems for the villages through a participatory process with the village members and village heads in group discussions and informal interviews respectively. The prototype systems developed by the village members were later validated by the key stakeholders through a one day community stakeholders’ workshop.
Through participatory methods, village members were given the space to identify existing institutions, organisations, groups and individuals that operate in their villages mainly on HIV/AIDS, general health and Gender Based Violence (GBV) issues. After identifying these stakeholders, community members were asked to point out those that have effective and active reporting structures through which community members themselves report health and GBV cases. Reporting structures such as village heads, village health workers, mothers groups, Community Based Organisations (CBOs) and religious leaders were identified during the exercise.

A community member draws a village map during a stakeholder mapping in Machinga district
At the community stakeholders’ workshop, mapped key stakeholders in the villages were invited to be part of the development of the community reporting systems through validation of the prototypes that were solicited from the community members, and to be informed about their roles in reporting social harms and who they will work with. Among other invited key stakeholders were village heads, CBOs, Faith Based Organisations (FBO), health workers, Health Surveillance assistants (HSAs), and community police, just to mention a few.
During the workshop, participants were briefed by the Research Assistants about the STAR-M project, potential social impacts of introducing HIVST, and the development of community reporting systems to be used in reporting social harms.
Social harms reporting system
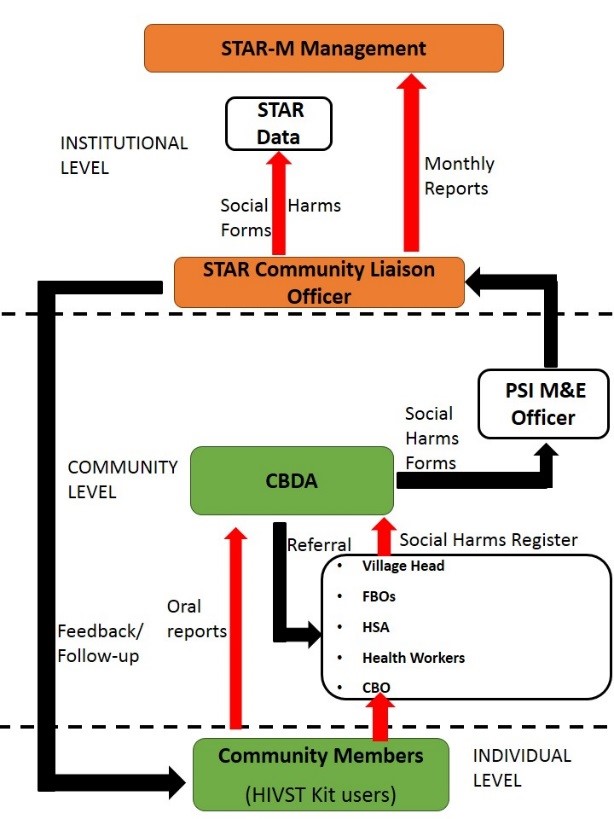 The social harms reporting systems in the participating villages will comprise of a number of components to ensure effective reporting of social harms cases. At the center of the systems at community level are Community Based Distribution Agencies (CBDAs) under Population Services International (PSI), which will be responsible for the distribution of HIVST kits in the communities, and identified community key stakeholders working on HIV/AIDS and GBV. Social harms victims will be able to report their cases direct to the CBDA or through the community based institutions/reporting structures. This is to allow flexibility in reporting, since different people in the communities open up to different institutions when it comes to reporting their concerns that have to be addressed. For instance, some open up to their faith leaders, village heads or their health workers. The community stakeholders will be liaising with the CBDA who will be recording the reported cases through a social harms reporting form that will then be sent through data collectors to MLW for records.
The social harms reporting systems in the participating villages will comprise of a number of components to ensure effective reporting of social harms cases. At the center of the systems at community level are Community Based Distribution Agencies (CBDAs) under Population Services International (PSI), which will be responsible for the distribution of HIVST kits in the communities, and identified community key stakeholders working on HIV/AIDS and GBV. Social harms victims will be able to report their cases direct to the CBDA or through the community based institutions/reporting structures. This is to allow flexibility in reporting, since different people in the communities open up to different institutions when it comes to reporting their concerns that have to be addressed. For instance, some open up to their faith leaders, village heads or their health workers. The community stakeholders will be liaising with the CBDA who will be recording the reported cases through a social harms reporting form that will then be sent through data collectors to MLW for records.
Social harms reporting systems will be established across the selected evaluation villages in the four districts and will include both intervention and control villages. The system in the control villages will be capturing social harms resulting from facility based testing, since HIVST will not be implemented there, and the one in the intervention villages will capture social harms resulting from HIVST and HIV testing and counseling. This will be used to make a comparison between facility based testing and HIVST on occurrence of social harms and serious adverse events.
The one-day workshops concluded with a training on how the CBDAs will be recording cases using the social harms reporting form and operation of the reporting systems. The exercise will proceed to the other two remaining districts of Blantyre and Mwanza where STAR-M is going to be implemented.

Research Assistants take a group photo with stakeholders after a workshop in Neno district

